You are here: Urology Textbook > Prostate > BPH > Symptoms
Benign Prostatic Hyperplasia (BPH): Signs and Symptoms
- Benign prostatic hyperplasia: definitions, epidemiology and etiology
- Benign prostatic hyperplasia: signs and symptoms
- Benign prostatic hyperplasia: diagnosis
- Benign prostatic hyperplasia: medical treatment
- Benign prostatic hyperplasia: surgical treatment
Review literature: (Burnett und Wein, 2006) (DGU guideline) (EAU guideline: Non-neurogenic male LUTS)
Lower Urinary Tract Symptoms of BPH
Storage symptoms:
Occur during the storage phase, previously termed as irritative symptoms: frequency, pollakiuria, nocturia, urgency, incontinence (urge, mixed or continuous, see below).
Causes of Storage Symptoms:
- The postvoid residual volume reduces the functional capacity of the bladder.
- Hypertrophy of the detrusor muscle causes an increased excitability.
- Age-related changes in the bladder and central nervous system: e.g., reduced cortical inhibition of the bladder sphincter and afferent bladder innervation.
- Higher probability of urinary tract infections.
Voiding symptoms:
Voiding symptoms were previously termed obstructive symptoms:
- Weak or spraying urinary stream
- Hesitancy: delayed begin of micturition
- Straining to urinate
- Intermittency: interrupted urine stream
- Terminal dribbling/li>
- Urinary retention
Causes of obstructive micturition symptoms:
Prostatic hyperplasia leads to the compression and narrowing of the prostatic urethra.
Overflow Urinary Incontinence:
BPH may cause different types of urinary incontinence: overflow urinary incontinence due to chronic urinary retention or urge incontinence due to detrusor instability. The surgical treatment of BPH includes the risk of developing stress urinary incontinence if the urinary sphincter is damaged.
Erectile Dysfunction:
Erectile dysfunction may be caused by BPH or its treatments (e.g., open prostatectomy, 5alpha-reductase inhibitors). The treatment of BPH, however, may also improve sexual function, e.g., alpha blocker such as doxazosin and phosphodiesterase inhibitors.
Complications of Benign Prostatic Hyperplasia
Urinary retention:
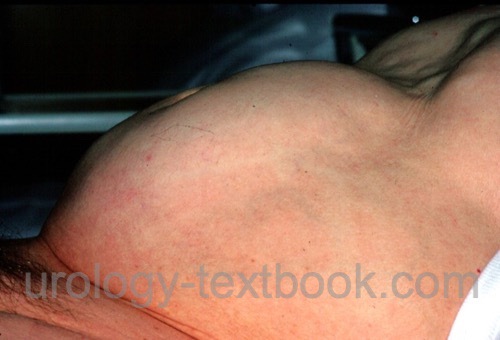
Risk factors for developing urinary retention are prostatitis, bladder overdistension, high fluid intake, alcohol, sexual activity, debility, drugs (e.g., sympathomimetics, anticholinergics), bed rest, surgery, and general anesthesia. The prognosis for the recovery of spontaneous voiding after urinary retention is better if the above-mentioned risk factors are present and the patient does not suffer from obstructive symptoms. In indolent patients, urinary retention may present as a lower abdominal tumor [fig. abdominal tumor due to urinary retention].
 |
Postrenal kidney failure:
BPH may lead to vesicoureteral reflux, hydronephrosis, and postrenal kidney failure. Uremia symptoms include lethargy, decreased mental acuity, coma, nausea, vomiting, bone pain, itch, shortness of breath, and seizures.
Further complications of Benign Prostatic Hyperplasia (BPH):
- Bladder diverticula
- Bladder stones
- Hematuria and bladder tamponade.
- Voiding with increased intra-abdominal pressure may cause hernias, hemorrhoids, or, rarely, micturition syncope.
- Urinary tract infections like prostatitis, pyelonephritis, or urosepsis.
Quantification of LUTS with the International Prostate Symptoms Score (IPSS)
The validated International Prostate Symptoms Score (IPSS) consists of 8 questions and is used to quantify BPH symptoms and to monitor treatment success. The IPSS, however, has no diagnostic value since other diseases like infections, neurogenic lower urinary tract dysfunction, or tumors may also cause high IPSS scores.
Evaluation of the IPSS:
The corresponding points of questions 1–7 are added together (total score 35 points). 0 to 7 points correspond to mild symptoms, 8 to 19 points to moderate symptoms, and 20 to 35 points to severe symptoms. The 8th question evaluates the quality of life and is reported separately to the total score.
1. Residual urine:
Over the past month, how often have you had a sensation of not emptying your bladder completely after you finish urinating?
- Not at all = 0 points
- Less than 1 time in 5 = 1 point
- Less than half of the time = 2 points
- About half of the time = 3 points
- More than half of the time = 4 points
- Almost always = 5 points
2. Frequency:
Over the past month, how often have you had to urinate again less than two hours after you finished urinating? (0–5 points, see classification residual urine)
3. Intermittency:
Over the past month, how often have you found you stopped and started again several times when you urinated? (0–5 points, see classification residual urine).
4. Urgency:
Over the last month, how difficult have you found postponing urination? (0–5 points, see classification residual urine)
5. Weak stream:
Over the past month, how often have you had a weak urinary stream? (0–5 points, see classification residual urine)
6. Straining during urination:
Over the past month, how often have you had to push or strain to begin urination? (0–5 points, see classification residual urine)
7. Nocturia:
Over the past month, how often did you most typically get up to urinate, from when you went to bed until you got up in the morning? (0–5 points depending on the times of nocturia)
8. Quality of life:
If you were to spend the rest of your life with your urinary condition the way it is now, how would you feel about that? [1–5 points: from delighted (0), pleased (1), mostly satisfied (2), mixed – about equally satisfied and dissatisfied (3), unhappy (4) and terrible (5)]
| BPH | Index | BPH diagnosis |
Index: 1–9 A B C D E F G H I J K L M N O P Q R S T U V W X Y Z
References
Andriole u.a. 2004 ANDRIOLE, G. L. ;
ROEHRBORN, C. ; SCHULMAN, C. ; SLAWIN, K. M. ;
SOMERVILLE, M. ; RITTMASTER, R. S.:
Effect of dutasteride on the detection of prostate cancer in men with
benign prostatic hyperplasia.
In: Urology
64 (2004), Nr. 3, S. 537–41; discussion 542–3
Burnett und Wein 2006 BURNETT, A. L. ; WEIN,
A. J.:
Benign prostatic hyperplasia in primary care: what you need to know.
In: J Urol
175 (2006), Nr. 3 Pt 2, S. S19–24
Chapple 2004 CHAPPLE, C. R.:
Pharmacological therapy of benign prostatic hyperplasia/lower urinary
tract symptoms: an overview for the practising clinician.
In: BJU Int
94 (2004), Nr. 5, S. 738–44
DGU Guideline, “S2e Leitlinie Diagnostik und Therapie des Benignen Prostatasyndroms (BPS).,” 2023. [Online]. Available: https://register.awmf.org/assets/guidelines/043-034l_S2e_Diagnostik_Therapie_benignes_Prostatasyndrom_2023-04.pdf
Donovan u.a. 2000 DONOVAN, J. L. ; PETERS,
T. J. ; NEAL, D. E. ; BROOKES, S. T. ; GUJRAL,
S. ; CHACKO, K. N. ; WRIGHT, M. ; KENNEDY, L. G. ;
ABRAMS, P.:
A randomized trial comparing transurethral resection of the prostate,
laser therapy and conservative treatment of men with symptoms associated with
benign prostatic enlargement: The CLasP study.
In: J Urol
164 (2000), Nr. 1, S. 65–70
“EAU Guideline: Non-neurogenic Male LUTS,” Available: https://uroweb.org/guidelines/treatment-of-non-neurogenic-male-luts/.
Kopp, R. P.; Freedland, S. J. & Parsons, J. K.
Associations
of benign prostatic hyperplasia with prostate cancer: the debate continues.
Eur
Urol, 2011, 60, 699-700; discussion 701-2.
Ørsted, D. D.; Bojesen, S. E.; Nielsen, S. F. &
Nordestgaard, B. G.
Association of clinical benign prostate hyperplasia
with prostate cancer incidence and mortality revisited: a nationwide
cohort study of 3,009,258 men.
Eur Urol, 2011, 60,
691-698.
Parsons, J. Kellogg; Messer, Karen; White, Martha;
Barrett-Connor, Elizabeth; Bauer, Douglas C; Marshall, Lynn M; in Men
(MrOS) Research Group, Osteoporotic Fractures & the Urologic Diseases in
America Project
Obesity increases and physical activity decreases lower
urinary tract symptom risk in older men: the Osteoporotic Fractures in Men
study.
Eur Urol, 2011, 60, 1173-1180.
Reich u.a. 2006 REICH, O. ; GRATZKE, C. ;
STIEF, C. G.:
Techniques and long-term results of surgical procedures for BPH.
In: Eur Urol
49 (2006), Nr. 6, S. 970–8; discussion 978
Uygur u.a. 1998 UYGUR, M. C. ; GUR, E. ;
ARIK, A. I. ; ALTUG, U. ; EROL, D.:
Erectile dysfunction following treatments of benign prostatic
hyperplasia: a prospective study.
In: Andrologia
30 (1998), Nr. 1, S. 5–10
 Deutsche Version: Symptome der benignen Prostatahyperplasie
Deutsche Version: Symptome der benignen Prostatahyperplasie