You are here: Urology Textbook > Testes > Epididymitis
Epididymitis
Definition, Classification and Etiology of Epididymitis
Acute or chronic inflammation of the epididymis of various etiologies:
- Bacterial epididymitis
- Epididymitis secondary to urinary tract infection: E. coli, Proteus, Klebsiella, Pseudomonas, Staphylococci
- Epididymitis secondary to sexually transmitted diseases: Chlamydia, Neisseria
- Tuberculosis: rare cause (hematogenous manifestation)
- Funiculitis: infection of the spermatic cord
- Nonbacterial infectious epididymitis: viral, fungal or parasitic etiology
- Noninfectious epididymitis: traumatic etiology, autoimmune, amiodarone-induced or idiopathic
- chronic inflammation of the epididymis longer than six weeks
- Chronic epididymalgia: chronic pain felt in the epididymis
Epidemiology of Epididymitis
Epididymitis is common, the incidence of epididymoorchitis in men aged 15–60 years is about 200–00/100.000.
Epididymitis: Signs and Symptoms
- Testicular pain and tenderness of the epididymis.
- Tender and swollen spermatic cord are signs of funiculitis.
- Scrotal swelling and redness.
- Intact cremasteric reflex. The Prehn sign is unreliable; it should be positive (lifting the testis alleviates the pain).
- fever indicates advanced infection.
- Complications: abscess, urosepsis, Fournier gangrene.
Diagnosis of Epididymitis
Urethral swab:
Urethral swab and PCR testing for gonorrhea or chlamydial infection if STD are possible.
Urine analysis:
- Urine sediment: leukocyturia.
- Urine culture: can identify the pathogen.
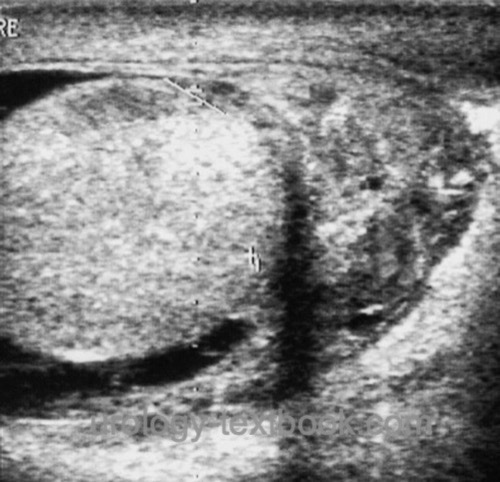
Testicular Ultrasound Imaging
Testicular ultrasound examination is mandatory for differential diagnosis of testicular torsion. In epididymitis, ultrasound imaging shows an enlarged epididymis, often with a hydrocele [ultrasound imaging: epididymitis]. It is important to identify abscess formation or signs of orchitis [ultrasound imaging: epididymoorchitis] and rule out testicular torsion with Doppler ultrasound.
 |
 |
 |
Surgical Exploration of the Scrotum
If there is doubt about the diagnosis of epididymitis, a surgical exploration of the scrotum is necessary to exclude testicular torsion. When a testicular tumor might be possible, an inguinal approach to the testis should be chosen.
Diagnosing voiding dysfunction
Uroflowmetry, exclusion of residual urine in the bladder, retrograde urethrography or cystogram are options to diagnose voiding dysfunction after healed epididymitis. Voiding dysfunctions are most likely in children or elderly patients with epididymitis.
Treatment of Epididymitis
Symptomatic Treatment
- Bed rest
- Elevation and cooling of the testes
- Anti-inflammatory drugs such as Diclofenac 75 mg 1-0-1
- Consider a nerve block of the spermatic cord at the external inguinal ring with a long-acting local anesthetic such as ropivacaine to successfully relieve significant pain.
Antibiotic Treatment of Epididymitis
After obtaining a urethral swab and urine culture, calculated antibiotic therapy is started in adolescents and adults. In children, bacterial infections of the epididymis are uncommon; some authors recommend antibiotic therapy only if there is evidence of a Urinary tract infections.
Suspected sexually transmitted epididymitis:
The IUSTI guideline recommends a single dose of ceftriaxone 1 g i.m. combined with azithromycin 2 g p.o. in a single dose. Ceftriaxone can also be administered i.v., the recommendation of the RKI is 1–2 g i.v. See also treatment of gonorrhea and treatment of non-gonococcal urethritis.
Epididymitis secondary to urinary tract infection:
Ciprofloxacin 500 mg 1-0-1 or other quinolones penetrate well into the epididymis and are prescribed for at least ten days. Alternatives are aminopenicillins with penicillinase inhibitor or oral cephalosporins. If necessary, correct the antibiotic depending on the urine culture result. In case of severe epididymitis with fever, choose intravenous therapy: ampicillin/clavulanic acid 2,2 g 1-1-1 i.v. or cephalosporin i.v. combined with gentamicin 3 mg/kgKG 1-0-0 i.v. or broad-spectrum antibiotics like imipenem or meropenem.
Surgical Therapy
| Do you want to see the illustration? Please support this website with a Steady membership. In return, you will get access to all images and eliminate the advertisements. Please note: some medical illustrations in urology can be disturbing, shocking, or disgusting for non-specialists. Click here for more information. |
- Epididymectomy: indicated in epididymitis refractory to antibiotic treatment or chronic epididymitis. Local complications are frequent (recurrent infections, impaired wound healing, loss of testicle)
- Orchiectomy: indicated in epididymoorchitis, abscess formation, and epididymitis refractory to antibiotic treatment as an alternative to epididymectomy.
| Testis, anatomy | Index | Mumps orchitis |
Index: 1–9 A B C D E F G H I J K L M N O P Q R S T U V W X Y Z
References
G. Bonkat, R. Bartoletti, F. Bruyère, S. E. Geerlings, F. Wagenlehner, and B. Wullt, “EAU Guideline: Urological Infections.” [Online]. Available: https://uroweb.org/guidelines/urological-infections/
Luzzi und O’Brien 2001 LUZZI, G. A. ; O’BRIEN,
T. S.:
Acute epididymitis.
In: BJU Int
87 (2001), Nr. 8, S. 747–55
 Deutsche Version: Epididymitis: Ursachen und Therapie
Deutsche Version: Epididymitis: Ursachen und Therapie